
江山代有才人出,各领风骚数百年。磺脲类叱咤风云60余载,今黑马SGLT2i崭露头角显现优势,疗效安全性究竟谁胜谁负,且听笔者为您细细道来。
来源 | 医学界内分泌频道
1时代变迁,更新换代
磺脲类药物是最早发现的口服降糖药物。1956年美国批准了第一个磺脲类药物甲苯磺丁脲上市,随着时代变迁,各种磺脲类药物不断进入临床,用于治疗2型糖尿病(T2DM)。目前磺脲类药物有60余载用药历史,其有效性及安全性不断提高,以格列本脲为代表的二代磺脲类在1966年上市,随后格列吡嗪、格列齐特、格列喹酮陆续上市。直到上世纪90年代,以格列美脲为代表的三代磺脲类上市,其更安全有效的优势得到普遍认可。
磺脲类药物通过磺酰脲基团与磺脲类受体1(SUR1)结合,使胰岛β细胞膜上的钾ATP通道关闭,抑制钾离子外流,导致β细胞膜去极化以及电压依赖的钙通道开放,钙离子内流,最终诱导含胰岛素的分泌颗粒释放。
而以达格列净为代表的钠-葡萄糖共转运蛋白2抑制剂(SGLT2i)是一种新型口服降糖药,其作用机制是非胰岛素依赖的。正常生理情况下,肾脏每天经过肾小球滤过约180g葡萄糖,而糖尿病病人每天过滤约280g葡萄糖。在肾小管内的葡萄糖主要通过钠-葡萄糖共转运蛋白(SGLT)重吸收回到血液循环中,其中SGLT2负责肾小管中90%葡萄糖的重吸收。SGLT2i通过抑制近端肾小管钠-葡萄糖重吸收,减少肾脏葡萄糖重吸收,促进尿糖排泄,而并非依赖促进胰岛素分泌机制降低血糖。
作为后起之秀的达格列净向老将磺脲类药物发起挑战,究竟踢馆结果如何?
2促泌降糖 PK 排糖降糖

Round 1
口服降糖药物,降糖效果最重要!
磺脲类药物降糖通过胰岛素依赖机制,单药治疗一般可降低糖化血红蛋白(HbA1C) 1-2%,平均降低1.5%【1】。有研究随访了应用磺脲类、噻唑烷二酮(TZD)类、二甲双胍等药物5年内β细胞功能的变化,结果表明患者β细胞功能逐年递减【2】。一般在1-2年内磺脲类可能出现失效,致HbA1c回升至治疗前水平【3】。而达格列净等SGLT2i类则为非胰岛素依赖机制,10mg达格列净单药治疗24周降低HbA1C约1.5%,与二甲双胍类似【4】。早期应用能显著改善胰岛β细胞功能、增加胰岛素敏感性。北京大学人民医院纪立农教授牵头了一项达格列净治疗亚洲T2DM的临床研究,其中89%患者来自中国,中国亚组数据表明,达格列净10mg组HOMA-2β细胞功能较安慰剂组平均增加11.85(6.18,17.52),HOMA-2IS(胰岛素敏感性)较安慰剂组平均增加16.21(10.07,22.36)【5】。格列美脲单药治疗血糖控制不佳的患者,加用达格列净后不仅可以进一步改善血糖,还能使体重得到控制【6】。
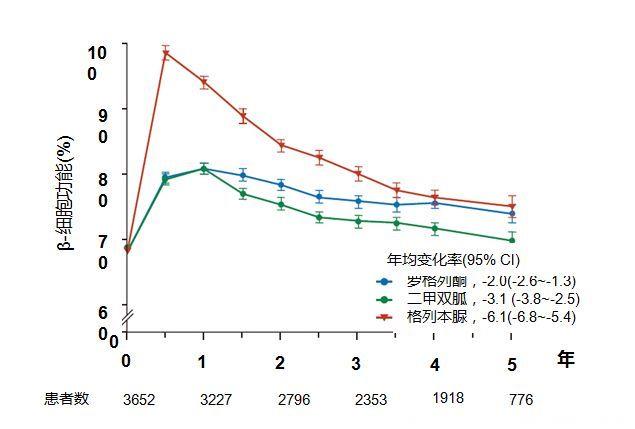
图1 各类降糖药物应用5年内β细胞功能变化情况【2】

Round 2
低血糖后果严重,必须关注!
低血糖是磺脲类药物治疗常见的不良反应,单药或联合用药时均可出现。为减少低血糖风险,应从小剂量开始,根据血糖结果调整药物剂量。而对达格列净而言,单药治疗时不增加低血糖发生风险,其低血糖风险与安慰剂类似【7】,与胰岛素或磺脲类药物联用时低血糖发生风险则会增加,此时应注意调整胰岛素或磺脲类药物的用量。亦有研究表明,斋月期间把降糖药物从磺脲类转换为达格列净能明显降低低血糖风险【8】。

Round 3
肥胖是万恶之源,谁能打败它?
磺脲类药物可引起患者体重增加,有研究表明,传统磺脲类药物(如格列本脲)对患者体重影响较大,治疗3年平均约增加3-5kg【9】;新型磺脲类或新剂型(如格列美脲或格列齐特缓释片)对患者体重影响较小,平均增加0.4-0.6kg【10,11】。而应用达格列净不但不增加体重,反而能助力体重控制、缩小腹围并减少内脏脂肪。中国数据表明,起始应用达格列净10mg 24周后体重较基线降低2.33kg【5】。国外数据表明,应用达格列净6个月腹围平均减少3.4cm,内脏脂肪平均减少13.9cm2【12】。
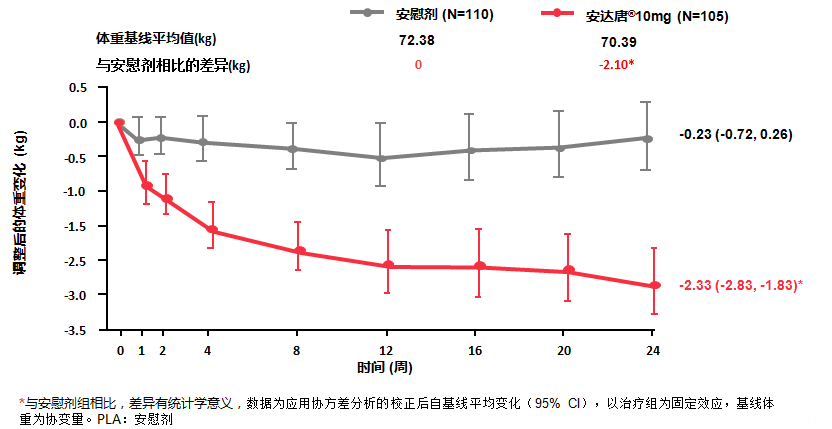
图2 达格列净及安慰剂应用24周内患者体重变化【5】

图3 达格列净应用6个月后患者内脏脂肪面积及腹围变化【12】

Round 4
明确心血管获益优势,更放心啦!
不同磺脲类药物心血管安全性存在差异,目前包括UKPDS、ADVANCE等多项大规模临床研究表明磺脲类药物治疗不增加心血管事件风险【13,14】,但在评估其心血管安全性仍需具体分析。里程碑式大型真实世界研究CVD-REAL研究表明:使用达格列净等SGLT2i治疗与降低糖尿病患者心血管死亡风险相关,使用达格列净等SGLT2i的患者全因死亡风险降低51%,心衰住院风险降低39%【15,16】。
3降糖利器,全新选择
磺脲类药物是目前治疗糖尿病领域应用最广泛的口服降糖药物之一,其应用历史悠久,具有相当重要的临床地位,其降糖作用强,但也具有增加体重、低血糖风险等副作用。关于磺脲类药物是否会增加心血管事件目前尚存争议。而以达格列净为代表的新药SGLT2i则另辟蹊径,通过非胰岛素依赖途径降糖并取得显著降糖效果。作为新型降糖药物,达格列净具有控制体重、低血糖风险罕见及可能有心血管获益的优势,已成为临床医生降糖药物的全新选择。
上期链接:降糖大作战!达格列净与二甲双胍XR疗效对比
除了与二甲双胍XR、磺脲类药物的疗效对比,SGLT2i抑制剂与α-葡萄糖苷酶抑制剂、DPP-4抑制剂等其他降糖药的PK未完待续,敬请期待哦!
参考文献:
【1】Hirst JA, et al. Estimating the effect of sulfonylurea on HbA1c in diabetes: a systematic review and meta-analysis. Diabetologia, 2013, 56:973-984
【2】TODAY Study Group, et al. A clinical trial to maintain glycemic control in youth with type 2 diabetes. N Engl J Med 2012;366(24):2247-56.
【3】Van Raalte DH, et al. Glucolipotoxicity and beta cells in type 2 diabetes mellitus: target for durable therapy? Diabetes Res Clin Pract. 2011 Aug;93 Suppl 1:S37-46.
【4】R.R.Henry, et al.Dapagliflozin, metformin XR, or both: initial pharmacotherapy for type 2 diabetes, a randomised controlled trial. Int J Clin Pract. 2012; 66(5):446-456.
【5】Ji L, et al. Dapagliflozin as monotherapy in drug-naive Asian patients with type 2 diabetes mellitus: a randomized, blinded, prospective phase III study. Clin Ther. 2014; 36(1):84-100.
【6】Strojek K, et al. Dapagliflozin added to glimepiride in patients with type 2 diabetes mellitus sustains glycemic control and weight loss over 48 weeks: a randomized, double-blind, parallel-group, placebo-controlled trial. Diabetes Ther, 2014,5(1): 267-283.
【7】Ferrannini E, et al. Dapagliflozin monotherapy in type 2 diabetic patients with inadequate glycemic control by diet and exercise: a randomized, double-blind, placebo-controlled, phase 3 trial. Diabetes Care, 2010,33: 2217-2224.
【8】Wan Seman, et al. Switching from sulphonylurea to a sodium-glucose cotransporter2 inhibitor in the fasting month of Ramadan isassociated with a reduction in hypoglycaemia. Diabetes Obes Metab, 2016,18(6): 628-32.
【9】United Kingdom Prospective Diabetes Study (UKPDS). 13: Relative efficacy of randomly allocated diet, sulphonylurea, insulin, or metformin in patients with newly diagnosed non-insulin dependent diabetes followed for three years.BMJ, 1995, 310(6972): 535-542.
【10】Schernthaner G, et al. GUIDE study: double-blind comparison of once-daily gliclazide MR and glimepiride in type 2 diabetic patients. Eur J Clin Invest,2004, 34(8):535-542.
【11】Guo XH, et al. Efficacy and safety of glimepiride as initial treatment in Chinese patients with Type 2 diabetes mellitus. Curr Med Res Opin, 2013, 29:169-174.
【12】Tosaki T, et al. Sodium-glucose Co-transporter 2 Inhibitors Reduce the Abdominal Visceral Fat Area and May Influence the Renal Function in Patients with Type 2 Diabetes.Intern Med. 2017;56(6):597-604.
【13】United Kingdom Prospective Diabetes Study (UKPDS). Intensive bloodglucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes(UKPDS 33). Lancet, 1998, 352(9131): 837-853.
【14】ADVANCE Collaborative Group, et al.Intensive blood glucose control and vascular outcomes in patients with type 2. N Engl J Med, 2008, 358(24):2560-2572.
【15】Kosiborod M, et al. Lower Risk of Heart Failure and Death in Patients Initiated on Sodium-Glucose Cotransporter-2 Inhibitors Versus Other Glucose-Lowering Drugs: The CVD-REAL Study (Comparative Effectiveness of Cardiovascular Outcomes in New Users of Sodium-Glucose Cotransporter-2 Inhibitors). Circulation. 2017 Jul 18;136(3):249-259.
【16】Birkeland KI, et al. Cardiovascular mortality and morbidity in patients with type 2 diabetes following initiation of sodium-glucose co-transporter-2 inhibitors versus other glucose-lowering drugs (CVD-REAL Nordic): a multinational observational analysis.lancet Diabetes Endocrinol. 2017 Sep;5(9):709-717.









